

cap-ONE

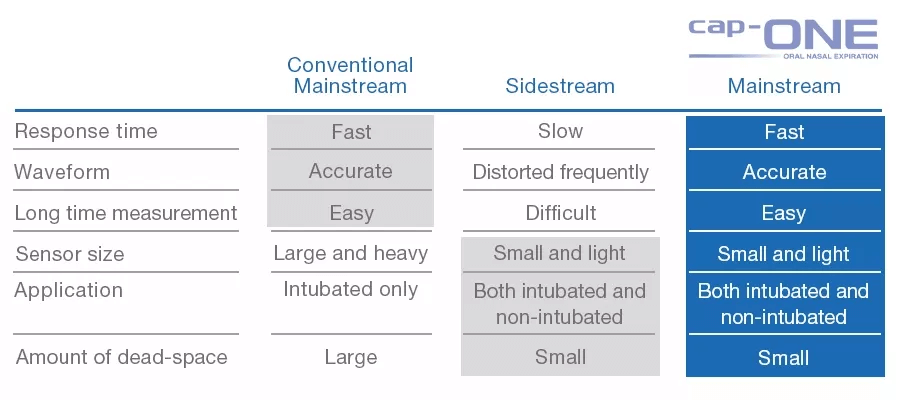
cap-ONE is Nihon Kohden's unique mainstream CO2 sensor for both intubated and non-intubated patients. The ultra compact sensor and unique adapter provide accurate measurements and reduce the burden on the patients. cap-ONE overcomes the disadvantages and maintains all the advantages of mainstream sensor for optimal capnography.
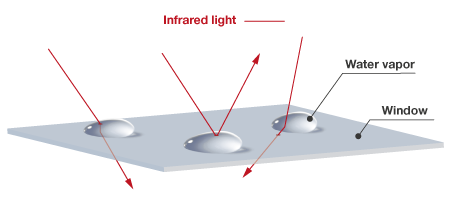
In the quantitative method, the infrared light transmitted through the airway adapter is split into two by a half mirror. One of which is detected as a signal output (Vs), the other passes through the gas cell* and is detected by another photo detector as the standard output (Vr). The partial pressure is calculated from the ratio of this signal output Vs and standard output Vr. *gas cell: a cell containing 100% CO2 gas
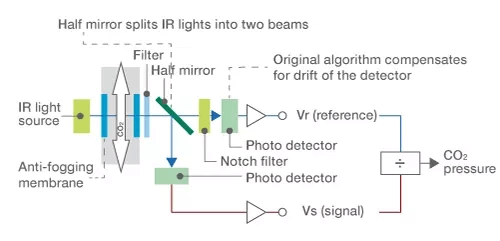
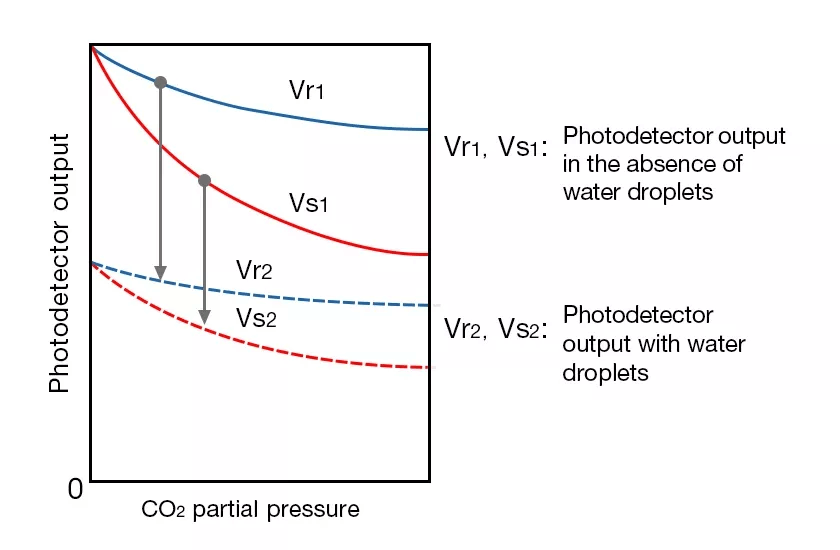
In the quantitative method, even the light intensity decreases, the ratio of signals and standard output (Vs/Vr) won’t change. Therefore, it is less likely to be affected by variables such as deterioration of light sources and dirty window of the sensor or water drops in the airway adapter and accurate CO2 partial pressure can be obtained. This measurement method is suitable for measurement when nebulizers are used or when humidification is used.

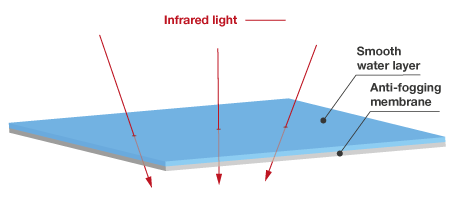
cap-ONE uses an original transparent film with an anti-fogging membrane. It forms a smooth layer of water which allows stable transmission of infrared light without irregular rejection. This technology eliminates the need for heaters and reduces the power consumption and weight of the sensor.
Without anti-fogging membrane | With anti-fogging membrane inside the airway |
|---|---|
 |  |
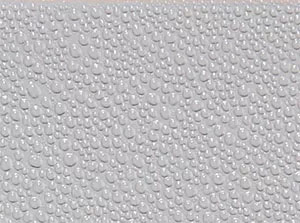 |  |
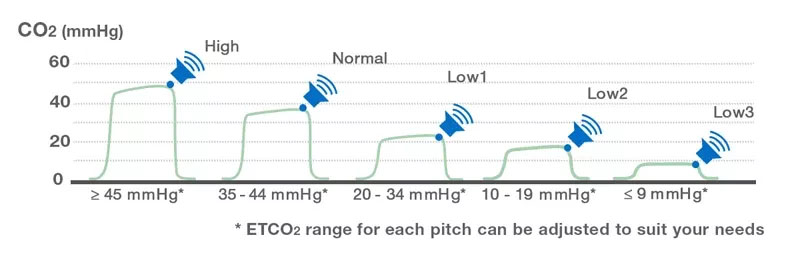
| Primarily designed for | ETCO2 Range | Sound Type | Sound Design | Example of Situation | Sound |
|---|---|---|---|---|---|
| Manual ventilation and ROSC confirmation | High 45≤ |  |  |
| |
| Normal 35-44 | 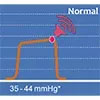 |  | Ventilation is sufficient | ||
| Low1 20-34 | 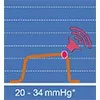 |  | Hyperventilation is caused by over aggressive manual ventilation during transport | ||
| CPR (Chest compression) | Low2 10-19 | 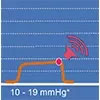 |  | High quality chest compressions are achieved | |
| Low3 ≤9 | 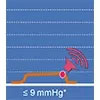 |  | Quality of effectiveness of chest compression may need improvement |
ROSC: Return of Spontaneous Circulation